Small Bowel Surgery
Small Bowel Surgery
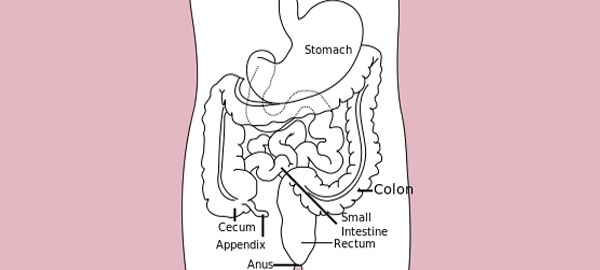
Surgical intervention on the bowel becomes necessary when a variety of serious conditions compromise the normal structure and function of the intestinal tract, including bowel cancer, diverticular disease, large polyps, impaired blood supply, and inflammatory bowel disease encompassing both Crohn's disease and ulcerative colitis. The specific surgical procedure performed depends entirely on the nature of the underlying condition and the extent of bowel involvement, with operations ranging from the removal of a small segment to the complete excision of the entire large bowel. These procedures carry distinct names reflecting the portion of bowel removed, including total colectomy for removal of the entire bowel, proctocolectomy for removal of the bowel along with the rectum and anus, hemicolectomy for removal of either the left or right side of the bowel, sigmoid colectomy for removal of the portion closest to the rectum, transverse colectomy for removal of the connecting segment joining both sides, and proctectomy for removal of the rectum and anus alone. Following bowel resection, the remaining ends of the bowel may be rejoined to restore continuity, or an artificial opening called a stoma may be created on the abdominal wall to allow waste to exit the body, a diversion that may be either temporary during the healing process or permanent depending on the extent of disease and the amount of bowel removed.
Surgery on the Small Intestine
Surgery on the small intestine represents one of the most frequently performed procedures in surgical practice, encompassing a broad spectrum of conditions that require either resection of a diseased segment or emergency intervention to address life-threatening complications. The small intestine, despite its seemingly protected position within the abdominal cavity, is vulnerable to a wide range of pathological processes including infection, inflammation, vascular compromise, malignancy, and traumatic injury, each of which may ultimately require surgical management. Small bowel obstruction surgery and small bowel resection surgery constitute the two most commonly performed categories of small intestinal operations, and the conditions leading to these interventions are diverse and clinically significant. A thorough understanding of the most common disease processes affecting the small intestine is essential for both timely diagnosis and the selection of the most appropriate surgical strategy to achieve the best possible patient outcomes.
Tuberculosis of the Intestine
Intestinal tuberculosis represents one of the most common indications for small bowel surgery in India, where the disease burden of tuberculosis remains significantly higher than in many other parts of the world. The small intestine, particularly the region of the distal small bowel and proximal colon known as the ileocaecal region, is the most frequently affected site of intestinal tuberculosis, a condition clinically referred to as ileocaecal tuberculosis. This condition typically presents with a progressive narrowing and obstruction of the bowel lumen caused by tuberculous inflammation and scarring, leading to a characteristic pattern of alternating constipation and diarrhea that worsens gradually over time as the obstruction becomes more complete. When medical anti-tubercular therapy alone proves insufficient to relieve the obstruction or when the degree of luminal narrowing becomes clinically significant, surgical treatment in the form of a limited resection of the ileocaecal region becomes necessary to restore normal intestinal continuity and relieve the obstructive symptoms that severely impair the patient's nutritional status and quality of life.
Small Bowel Perforation
Small bowel perforation, most commonly caused by typhoid ulcers that erode through the full thickness of the intestinal wall, represents one of the most serious and immediately life-threatening emergencies encountered in abdominal surgery. When a typhoid ulcer perforates, intestinal contents spill freely into the peritoneal cavity, causing a severe and rapidly spreading infection of the abdominal lining known as peritonitis, which can progress to septic shock and death if not surgically addressed with absolute urgency. This condition demands emergency laparotomy — an urgent surgical opening of the abdomen — followed by thorough washout of the peritoneal cavity and primary closure of the perforation site to prevent continued contamination. The management of typhoid perforation requires not a moment of delay, as every hour that passes without surgical intervention dramatically worsens the degree of peritoneal contamination, increases the systemic inflammatory response, and significantly reduces the patient's chances of survival and uncomplicated recovery.
Bleeding from the Small Bowel
Bleeding originating from the small bowel is an uncommon yet diagnostically challenging condition that is frequently categorized as obscure gastrointestinal bleeding, a term reflecting the significant difficulty clinicians face in identifying its precise source within the lengthy and relatively inaccessible small intestinal tract. The clinical presentation of small bowel bleeding spans a wide spectrum, ranging from slow chronic oozing that manifests as gradual anemia and intermittently positive stool tests, to sudden massive hemorrhage that constitutes an acute life-threatening emergency requiring immediate resuscitative measures. Because the small bowel lies beyond the reach of conventional upper and lower endoscopy, its evaluation requires specialized diagnostic modalities including capsule endoscopy — in which the patient swallows a tiny camera-equipped capsule that photographs the entire intestinal lining — enteroscopy using specialized long-reach endoscopes, and nuclear medicine scanning techniques that can detect and localize active bleeding sites. Once the precise location of the bleeding source has been accurately identified through these investigations, surgical resection of the affected segment of small bowel becomes necessary to achieve definitive control of the hemorrhage and prevent potentially fatal recurrence.
Crohn's Disease
Crohn's disease is a chronic inflammatory condition of the gastrointestinal tract that is being encountered with increasing frequency in clinical practice, predominantly affecting young individuals and presenting with a characteristic pattern of chronic diarrhea, abdominal pain, and progressive unintentional weight loss that can profoundly impact the patient's physical health and overall well-being. Modern advances in diagnostic technology have made accurate identification of Crohn's disease considerably more reliable, with specific investigations including colonoscopy with biopsy, capsule endoscopy, MRI enterography, and specialized blood and stool markers now available to confirm the diagnosis and assess the extent of intestinal involvement. The majority of patients with Crohn's disease are managed primarily through long-term medical treatment using anti-inflammatory agents, immunosuppressants, and biological therapies aimed at inducing and maintaining remission and preventing disease progression. However, a significant proportion of patients eventually develop serious complications including bowel obstruction caused by inflammatory strictures and internal fistulae — abnormal channels connecting loops of bowel to adjacent organs — that fail to respond to medical therapy and necessitate repeated surgical interventions throughout the patient's lifetime.