Liver Surgery
Liver Abscess
A liver abscess is a pus-filled cyst that develops within the liver, one of the body's most vital organs responsible for producing bile to aid digestion, creating essential hormones and substances, filtering toxins from the blood including those from alcohol and medications, and regulating fat storage and cholesterol production. The condition can affect anyone and arises through various pathways, including infections that spread directly from nearby structures such as the bile-draining tubes, the appendix, or the intestines, as well as infections carried through the bloodstream from more distant parts of the body. Liver abscesses can also develop as a complication of surgery or physical trauma to the liver. The most common forms are bacterial — known as pyogenic liver abscess — and parasitic, particularly amebic liver abscess caused by microscopic organisms called amebas, the same organisms responsible for the intestinal disorder amebic dysentery.
When identified early, a liver abscess is typically treatable and curable through a course of antibiotics alone or in combination with a surgical drainage procedure. However, if left undetected or untreated, the abscess can rupture and spread the infection throughout the body, leading to sepsis, a life-threatening condition involving bacterial infection of the bloodstream. The symptoms of liver abscess are varied and can include upper right abdominal pain, fever or chills, nausea, diarrhea, dark urine, clay-colored stools, joint pain, unexplained weight loss, loss of appetite, and jaundice — a yellowing of the skin and whites of the eyes. In more critical situations, life-threatening symptoms may emerge such as sudden confusion or behavioral changes, high fever exceeding 101 degrees Fahrenheit, rapid heart rate, severe breathing difficulties, jerky movements, and extreme lethargy, all of which demand immediate emergency medical attention without delay.
Liver Cyst
Liver cysts are thin-walled, fluid-containing structures that occur in approximately five percent of the general population, though only about five percent of those affected ever develop noticeable symptoms. Most liver cysts are single in nature, although some patients may present with multiple cysts scattered throughout the liver. When symptoms do occur, they commonly include upper abdominal fullness, discomfort, or a dull aching pain in the right upper region of the abdomen. In a small number of cases, bleeding can occur into the cyst, causing sudden and severe pain in the right upper quadrant that may radiate to the shoulder, though this bleeding typically resolves on its own over several days with gradual improvement in pain. Importantly, liver cysts do not impair the liver's functional capacity and are almost always benign, with diagnosis typically confirmed through ultrasound or CT scanning.
Treatment for liver cysts is only necessary in patients who develop significant symptoms, as most cysts remain harmless and require no intervention. Simple needle aspiration to drain the fluid is generally ineffective because the cyst invariably refills within days, making surgical removal of a large portion of the cyst wall the preferred and most durable treatment approach. This procedure is most commonly performed laparoscopically through just two to three small incisions, requiring only an overnight hospital stay with full recovery expected within two weeks and a very low risk of recurrence. A rare subset of the population — approximately 0.6 percent — develops polycystic liver disease, a condition in which the liver becomes massively enlarged and resembles a cluster of very large grapes, causing severe abdominal swelling, chronic pain, and a dramatically reduced quality of life. Unlike polycystic kidney disease, polycystic liver disease does not cause liver failure, but in extreme cases where suffering becomes unmanageable, liver transplantation remains the only definitive long-term solution available to affected patients.
Cystic Tumors
Cystic tumors of the liver are fundamentally different from simple liver cysts in that they represent actual tissue growths with the potential to become malignant over the course of many years if not identified and treated appropriately. The most commonly encountered benign form is called a cystadenoma, a slow-growing cystic tumor that, if left untreated, carries the risk of transforming into its malignant counterpart known as a cystadenocarcinoma. The symptoms produced by cystic tumors closely resemble those of simple cysts, presenting as upper abdominal fullness, discomfort, and pain, making clinical differentiation between the two conditions difficult on symptoms alone. Liver blood tests typically remain within normal ranges unless a malignancy has already developed, and the most reliable diagnostic tools are ultrasound and CT scanning, which reveal the characteristic mixed composition of these tumors containing both liquid and solid areas within the same lesion.
Because of the inherent risk of malignant transformation, cystic tumors of the liver must always be completely and surgically removed, requiring an open operative approach rather than laparoscopic surgery to ensure thorough excision and minimize the risk of leaving residual tumor tissue behind. Complete surgical removal is critical not only to eliminate the existing tumor but also to prevent the possibility of cancerous progression that would significantly worsen the patient's long-term prognosis. Fortunately, the recurrence rate following complete surgical resection is very low, and patients who undergo successful removal of a cystic tumor — whether benign or early-stage malignant — generally enjoy an excellent long-term outlook. Early detection therefore plays an indispensable role in the management of these lesions, as tumors identified and removed before malignant transformation has occurred offer patients the best possible chance of a full and lasting recovery with minimal risk of the disease returning.
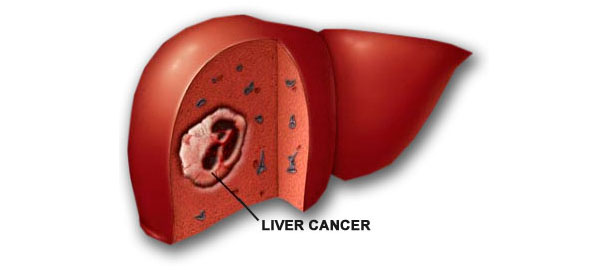
Liver Cancer
Liver cancer is a malignancy that originates within the cells of the liver itself, a football-sized organ situated in the upper right portion of the abdomen, nestled beneath the diaphragm and above the stomach. The most prevalent form is hepatocellular carcinoma, which arises from hepatocytes, the main functional cells of the liver, though other cell types within the liver can also undergo malignant transformation albeit far less commonly. It is important to distinguish primary liver cancer from metastatic cancer, which originates in another organ such as the colon, lung, or breast and subsequently spreads to the liver — such cancers are named after their organ of origin and are classified and treated differently from true liver cancer. Liver cancer develops when liver cells acquire mutations in their DNA, the molecular blueprint governing all cellular processes, causing affected cells to grow uncontrollably and accumulate into a tumor mass capable of invading surrounding tissue and spreading to other parts of the body.
One of the most challenging aspects of liver cancer is that most patients experience no signs or symptoms during the early stages of the disease, allowing it to progress silently until it reaches an advanced and more difficult-to-treat stage. When symptoms do eventually appear, they typically include unintentional weight loss, loss of appetite, upper abdominal pain, nausea and vomiting, general weakness and fatigue, abdominal swelling, jaundice manifesting as a yellow discoloration of the skin and whites of the eyes, and white or chalky stools. While the precise cause of most liver cancers remains unclear, chronic infection with certain hepatitis viruses is one of the best-established and most well-recognized contributing factors in the development of this disease. Early detection through regular screening of high-risk individuals remains the most effective strategy for improving survival outcomes in liver cancer patients.
Hydatid Cysts of the Liver
Hydatid cyst disease is a parasitic infection caused by Echinococcus, a tapeworm parasite whose larvae invade the body and form fluid-filled cystic cavities most commonly within the liver, though other organs can also be affected. One of the most clinically significant features of this condition is its remarkably prolonged silent phase, during which an infected individual may remain completely asymptomatic for anywhere between ten and twenty years while the cyst slowly enlarges to a detectable size. Once the cyst becomes large enough to exert pressure on surrounding structures or triggers an inflammatory response, patients may begin to experience pain in the upper right abdomen, persistent itching, fever, chest pain, or cough. In complicated cases where the cyst ruptures, becomes infected, or compresses adjacent bile ducts or blood vessels, more severe presentations can occur including jaundice, high fever, and coughing up blood-tinged sputum, all of which signal the need for urgent medical intervention.
The management of hydatid cysts depends on their size, location, complexity, and response to treatment, with medical therapy being the first line of approach in many cases. Anti-parasitic medications such as albendazole or mebendazole, administered for up to three months, form the cornerstone of medical treatment, and the addition of praziquantel to either agent may enhance therapeutic efficacy in select patients. However, when cysts fail to respond adequately to medical therapy or develop serious complications, surgical removal becomes necessary to achieve definitive cure. The most complete and effective surgical approach is cysto-pericystectomy, which involves the total removal of the cyst along with its surrounding tissue, offering the best possible chance of complete eradication of the infection with the lowest risk of recurrence compared to more conservative surgical techniques.
Liver Injury
A liver injury refers to any form of physical damage sustained by the liver as a result of trauma, with the most common presentation being a bruise or contusion to the organ caused by blunt force impact to the abdomen. More severe injuries may involve lacerations — actual tears in the liver tissue — which carry a significantly higher risk of life-threatening hemorrhage given the liver's exceptionally rich blood supply and its critical role in the body's circulatory system. The clinical presentation of a liver injury can range from mild and localized discomfort to a full systemic emergency, with symptoms including right upper abdominal pain and tenderness, abdominal swelling, blood in the stool or urine, vomiting, jaundice, brown discoloration of the urine, and cardiovascular signs of internal bleeding such as rapid pulse, faintness, and fainting.
The treatment strategy for a liver injury is determined entirely by the severity and extent of the damage sustained. Minor contusions and small lacerations that are not actively bleeding may be managed conservatively with careful observation, rest, and supportive care, as the liver possesses a remarkable capacity for self-repair and regeneration when the injury is limited in scope. In contrast, severe lacerations accompanied by significant hemorrhage or structural disruption of the liver require prompt surgical intervention to control bleeding, repair damaged tissue, and prevent the potentially fatal complications of uncontrolled internal blood loss. Advances in both surgical technique and interventional radiology have greatly improved survival outcomes for patients with serious liver trauma, though rapid diagnosis, timely transfer to a specialized surgical center, and swift operative decision-making remain the most critical determinants of a successful recovery.