Esophageal Surgery
Surgery for Corrosive Esophageal Injury
Caustic ingestion poses a serious and potentially life-threatening danger to the esophagus and stomach. The severity and extent of damage depend on several key factors, including the corrosive properties of the ingested substance, the amount, concentration, and physical form — whether solid or liquid — of the agent, and the duration of contact with the mucosal lining. These variables collectively determine how deeply the caustic material penetrates the esophageal wall and how extensive the resulting tissue destruction will be. Understanding these factors is essential for clinicians in assessing injury severity and planning appropriate surgical or medical intervention.
The demographic profile of caustic ingestion victims varies significantly between accidental and intentional cases. Most ingestions occur in children, who frequently expectorate much of the caustic agent before swallowing, thereby minimizing the degree of injury. The remaining cases involve psychotic, suicidal, and alcoholic subjects, who tend to ingest larger quantities of caustic agents and are therefore more likely to suffer severe esophageal and gastric damage. More than 5,000 caustic ingestions are reported annually in the United States alone, making it the leading cause of esophageal strictures in children. Prevention remains a critical public health priority, particularly in developing countries where such injuries are largely unreported and access to timely surgical care is limited.
Esophageal Cancer
Esophageal cancer is a malignancy that originates in the cells lining the inner surface of the esophagus, the long hollow tube that runs from the throat to the stomach and carries swallowed food for digestion. It can arise anywhere along the length of the esophagus, though in the United States it most frequently occurs in the lower portion. The disease affects men more commonly than women and is classified into distinct types based on the cell of origin. Adenocarcinoma, which begins in mucus-secreting gland cells, is the most common form in the United States and predominantly affects white men, while squamous cell carcinoma, arising from the flat surface-lining cells of the mid-esophagus, remains the most prevalent type worldwide. Rare forms such as choriocarcinoma, lymphoma, melanoma, sarcoma, and small cell cancer also exist but are far less frequently encountered.
The clinical presentation of esophageal cancer ranges from completely asymptomatic in its early stages to increasingly debilitating as the disease advances. Common symptoms include progressive difficulty swallowing (dysphagia), unintentional weight loss, chest pain or pressure, fatigue, frequent choking while eating, indigestion or heartburn, and coughing or hoarseness. Because early-stage disease typically produces no warning signs, diagnosis is often delayed until the tumor has grown significantly.
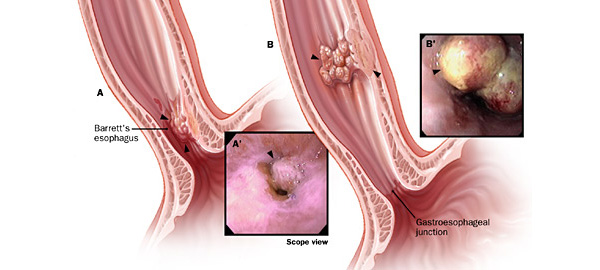
The underlying cause involves DNA mutations in esophageal cells that trigger uncontrolled growth and division, forming a tumor capable of invading nearby structures and metastasizing to distant parts of the body. Chronic irritation of the esophageal lining is considered a major driver of these mutations, with well-established risk factors including alcohol consumption, smoking, tobacco chewing, gastroesophageal reflux disease (GERD), Barrett's esophagus, obesity, bile reflux, achalasia, radiation therapy to the chest, drinking very hot liquids, diets low in fruits and vegetables, and consumption of foods preserved in lye.
Surgery for cancer of GE Junction
Gastroesophageal cancer is a silent and insidious disease that disproportionately affects populations in the South, preying particularly on individuals who have long relied on alcohol and tobacco as part of their daily lives. Unlike many other cancers that present with early warning signs, this malignancy develops slowly at the junction between the esophagus — the tube connecting the mouth to the stomach — and the stomach itself, making early detection extraordinarily difficult. A typical patient seeks medical attention only after experiencing dysphagia, or difficulty swallowing, accompanied by notable weight loss, often after months of gradual symptom progression lasting anywhere from one to six months. Many patients find themselves unable to swallow solid food while managing liquids, or in some cases the reverse, yet most consider themselves otherwise healthy individuals with no significant family history or recognized risk factors. Tragically, nearly all arrive at their physician's office fully expecting a simple prescription to resolve their condition, unaware of the serious and complex disease process already well underway within their bodies. Recent statistics and clinical observations suggest that this disease is not only becoming more common but also more aggressive than historical data would have previously indicated, raising serious concern among oncologists and surgeons alike.
The biological foundation of gastroesophageal cancer lies in a well-established multistage process recognized by cancer researchers worldwide, consisting of an initiation phase and a promotion phase. The initiation phase begins when a carcinogen — typically an alkylating agent or chemical irritant such as those found in tobacco smoke, alcohol, or acidic reflux — attacks and damages the cellular wall of the esophagus or stomach. This initial injury may heal naturally without consequence, but when the cellular repair mechanisms fail or are overwhelmed by repeated insults, permanent structural changes occur at the cellular level, setting the stage for malignant transformation. The promotion phase then follows, characterized by the injured cells beginning to proliferate at a rate faster than the surrounding normal tissue, producing what is known as an in situ or early-stage tumor confined to a superficial layer of tissue. This progression follows a predictable but dangerous sequence: normal tissue gives way to hyperplasia, an abnormally rapid growth of otherwise normal-appearing cells, which then transitions into dysplasia, where the cells begin to appear structurally abnormal under microscopic examination, ultimately culminating in early invasive cancer and finally full-blown metastatic disease capable of spreading to distant organs throughout the body.
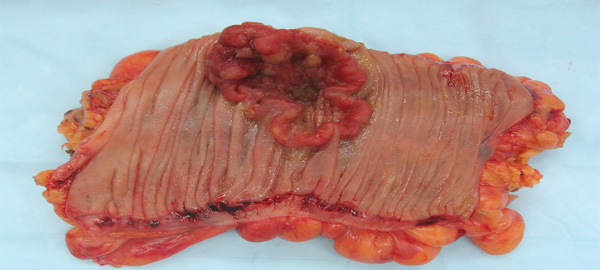
The cellular origin of gastroesophageal cancers further defines their clinical behavior and guides treatment strategy. Historically, the two dominant cell types are squamous cell carcinoma, which arises from the lining of the esophagus and predominates in the upper and middle portions, and adenocarcinoma, which develops from the glandular lining of the stomach and is most commonly found at the gastroesophageal junction and lower esophagus. Both carry significant morbidity and mortality, particularly when diagnosed at an advanced stage, which remains the norm given the disease's silent early course. However, clinicians are increasingly encountering unusual cellular variants derived from other cell lines, all presenting with remarkably similar clinical pictures yet potentially differing in their response to therapy and overall prognosis. This evolving landscape of tumor biology underscores the growing complexity of managing gastroesophageal cancer and highlights the urgent need for improved screening strategies, heightened public awareness, and more aggressive early intervention — particularly in high-risk populations who continue to engage in the very behaviors that initiate and promote this devastating disease process.
Achalasia cardia
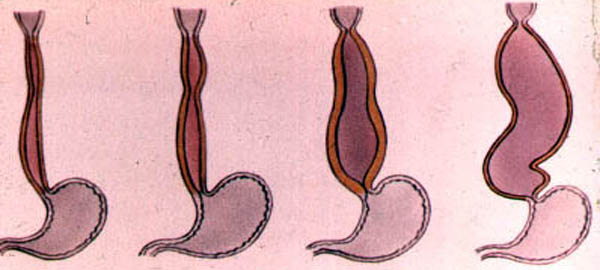
Achalasia cardia is a rare but significant disease affecting the muscular structure of the esophagus, the hollow swallowing tube that connects the throat to the stomach. The term "achalasia" itself is derived from Greek, meaning "failure to relax," and this definition precisely captures the central pathological problem of the condition. The disease is characterized by the inability of the lower esophageal sphincter — a specialized ring of muscle located at the junction between the lower esophagus and the stomach — to open and allow food to pass freely into the stomach during swallowing. This functional failure results in the progressive accumulation of food and liquid within the esophagus, leading to the constellation of symptoms that define this condition. While achalasia can affect individuals of any age or gender, it remains relatively uncommon in the general population, making awareness and early recognition by both patients and clinicians critically important for timely diagnosis and effective management.
How does the normal esophagus function?
The esophagus has three functional parts. The uppermost part is the upper esophageal sphincter, a specialized ring of muscle that forms the upper end of the tubular esophagus and separates the esophagus from the throat. The upper sphincter remains closed most of the time to prevent food in the main part of the esophagus from backing up into the throat. The main part of the esophagus is referred to as the body of the esophagus, a long, muscular tube approximately 20 cm (8 in) in length. The third functional part of the esophagus is the lower esophageal sphincter, a ring of specialized esophageal muscle at the junction of the esophagus with the stomach. Like the upper sphincter, the lower sphincter remains closed most of the time to prevent food and acid from backing up into the body of the esophagus from the stomach.
The upper sphincter relaxes with swallowing to allow food and saliva to pass from the throat into the esophageal body. The muscle in the upper esophagus just below the upper sphincter then contracts, squeezing food and saliva further down into the esophageal body. The ring-like contraction of the muscle progresses down the body of the esophagus, propelling the food and saliva towards the stomach. (The progression of the muscular contraction through the esophageal body is referred to as a peristaltic wave.). By the time the peristaltic wave reaches the lower sphincter, the sphincter has opened, and the food passes into the stomach.
The most common symptom of achalasia is difficulty in swallowing (dysphagia). Patients typically describe food sticking in the chest after it is swallowed. Dysphagia occurs with both solid and liquid food. Moreover, the dysphagia is consistent, meaning that it occurs during virtually every meal.
Sometimes, patients will describe a heavy sensation in their chest after eating that may force them to stop eating. Occasionally, pain may be severe and mimic heart pain (angina). The cause of this discomfort is felt to be the accumulation of ingested food within the esophagus.
Regurgitation of food that is trapped in the esophagus can occur, especially when the esophagus is dilated. If the regurgitation happens at night while the patient is sleeping, food can enter the throat and cause coughing and choking. If the food enters the trachea (windpipe) and lung, it can lead to infection (aspiration pneumonia).
There was some preliminary evidence that treatments by specialist staff working in primary.There was some preliminary evidence that treatments by specialist staff working in primary.Your childs primary and permanent treatment is important to help your child establish good oral